LETTER TO THE EDITOR | https://doi.org/10.5005/jp-journals-10071-23891 |
Check Central Venous Catheter Set thoroughly or Bite the Bullet!
1,2,4Department of Anaesthesia, Pain Medicine and Critical Care, All India Institute of Medical Science, New Delhi, India
3Critical and Intensive Care, JPNA Trauma Centre, All India Institute of Medical Science, New Delhi, India
Corresponding Author: Richa Aggarwal, Critical and Intensive Care, JPNA Trauma Centre, All India Institute of Medical Science, New Delhi, India Phone: +91 919873731042, e-mail: pathakricha@yahoo.co.in
How to cite this article: Singh AK, Kumar S, Aggarwal R, Trikha A. Check Central Venous Catheter Set thoroughly or Bite the Bullet! Indian J Crit Care Med 2021;25(7):832–833.
Source of support: Nil
Conflict of interest: None
Sir,
Resistance during guidewire insertion in central venous cannulation is not uncommon. It may occur due to anatomical difficulty like venous valve, some technical difficulty like manufacturing defect in central venous catheter (CVC) set, or sometimes when the procedure is being done by inexperienced hands. We report a case in which we encountered resistance in guidewire negotiation due to an unusual defect in the introducer needle of CVC set (Certofix Trio standard V set) and suggest revising the checklist before insertion of central line to detect the same.
A 55-year-old man, known case of chronic liver disease with portal hypertension, hepatic encephalopathy grade 2 and ascites, and COVID-19 (RT-PCR positive), was admitted to COVID-19 intensive care unit (ICU) with two episodes of hematemesis from the ward. On admission, he was drowsy with a pulse rate of 130 beats/minute, a blood pressure 96/56 mm Hg on noradrenaline infusion at the rate of 0.1 µ/kg/min, and oxygen saturation of 90% at room air. He was intubated in view of threatened airway. His basic lab parameters were as follows: Hb—5.6; TLC—6600; platelet count—80,000; INR—4.6; serum bilirubin—8.2; SGOT/SGPT—163/216; urea—76; creatinine—5.2; serum Na—127; and serum K—4.7. The management was started according to the standard hospital protocol. In view of vasopressor support, ultrasound-guided right internal jugular vein (IJV) cannulation was planned keeping in mind the risk of bleeding due to deranged coagulation and thrombocytopenia. After proper positioning and complete aseptic precaution, the right IJV was identified with the help of a high-frequency linear probe of ultrasound. After local anesthetic infiltration, under real-time ultrasound, right IJV was punctured and guidewire insertion tried through Y-connector of the needle. There was some resistance in insertion and only 5 cm of the guidewire could be negotiated. After a while of unsuccessful negotiation, we decided to remove the guidewire but it was stuck inside the needle. We removed needle–guidewire assembly as a whole and pressed the insertion site to avoid bleeding. After removal of whole conduit, we tried to pull out the guidewire but could not as it was stuck somewhere around the valve part (Fig. 1). We manually straightened the J-part of guidewire and tried to negotiate, but we failed. Then we pulled a little harder, and it opened like a spring (Fig. 1) and came out. Thereafter, we opened the new catheter set and could cannulate IJV easily in one go.
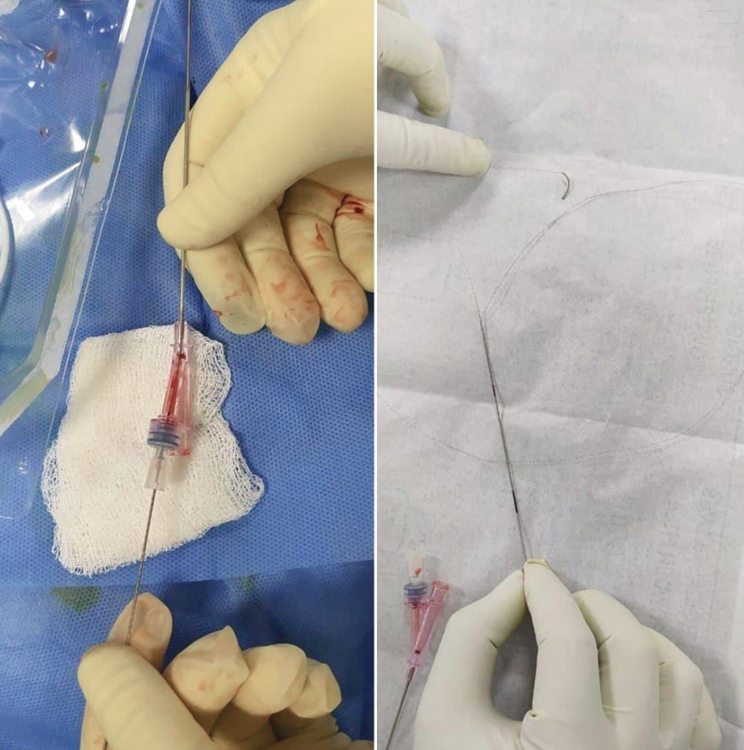
Fig. 1: Guidewire stuck at hub (L), and after applying some force, it opened like spring (R)
Choudhury et al.1 were confronted with similar situation and they also removed needle–guidewire assembly together. In their case, resistance was due to impacted small piece of tissue inside the introducer needle. In our case, the guidewire was stuck similarly and we tried to remove the guidewire by maneuver described by Arya et al.2 We could not retrieve even by rotating the guidewire or needle by 90 to 180° mainly because in our case, the guidewire was stuck at the hub of Y-piece and not at the tip. Similarly, the technique described by Henderson3 did not work because the needle could not be retrieved over the guidewire.
Manufacturing defects in CVC sets are sporadic events but they can cause serious mishaps, such as broken guidewire tip and its embolization, multiple punctures leading to pneumothorax, and large hematoma. We would like to emphasize on revising the simplified preprocedural checklist described by Gandhi et al.4, highlighting the last point that says about the ability to negotiate the guidewire through introducer needle using a dispenser. So an ounce of prevention is worth a pound of cure; this way we can further minimize procedure-related complications, especially in cases with deranged coagulation.
ORCID
Ashutosh K Singh https://orcid.org/0000-0002-4421-8090
Sandeep Kumar https://orcid.org/0000-0001-7641-8807
Richa Aggarwal https://orcid.org/0000-0002-4531-2759
Anjan Trikha https://orcid.org/0000-0002-6001-8486
REFERENCES
1. Choudhury A, Agarwal A, Dhiraaj S. An unusual case of guidewire impaction during internal jugular venous cannulation. Anesth Analg 2005;100(4):1217–1218. DOI: 10.1213/01.ANE.0000149012.22125.B8.
2. Arya VK, Kumar A. Technique of retrieval of J-tip guidewire without withdrawing introducer needle during central venous cannulation by Seldinger technique. Anesth Analg 2004;98(2):553–554. DOI: 10.1213/01.ane.0000077711.21575.95.
3. Henderson JJ. Failure to advance the guidewire when the Seldinger technique is used for central venous cannulation: safe and reliable recovery. Anesth Analg 2004;99(2):620–630. DOI: 10.1213/01.ANE.0000130910.46642.52.
4. Gandhi KA, Samra T. Preprocedural check of central venous catheter set. Indian J Crit Care Med 2018;22(3):197–198. DOI: 10.4103/ijccm.IJCCM_360_17.
________________________
© The Author(s). 2021 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.